

If you’ve ever had your skin checked by a doctor and noticed them press a small device with a light up against your mole, you’ve witnessed dermoscopy in action. Most patients have no idea what that little tool does or why it matters so much.
Here’s what’s actually going on, explained in plain terms.
What Is Dermoscopy?
Dermoscopy is a technique that lets doctors examine the skin in much greater detail than the naked eye allows. Using a handheld device called a dermatoscope, the doctor can see patterns, structures, and colours within a mole that are completely invisible without magnification.
The term comes from the Greek words for ‘skin’ (derma) and ‘to look’ (skopein). It’s been used in dermatology for several decades, but the quality of the instruments and the training of the doctors who use them has improved enormously in recent years.
What Does a Dermatoscope Actually Do?
A dermatoscope is essentially a powerful magnifying lens combined with a light source. When placed against the skin (usually with a small amount of contact fluid or ultrasound gel), it reduces the surface reflection of the skin that would otherwise scatter and distort the light. This is called immersion dermoscopy.
Modern versions also use cross-polarized light, a technology that eliminates surface glare without needing gel. This is more convenient in a clinical setting and is now standard in most quality instruments.
The result is that the doctor can see features that sit beneath the very top layer of skin, the epidermis. These include pigment networks, blood vessel patterns, the distribution of melanin (the pigment that gives moles their color), and structural features that are highly specific to different types of skin lesions.
Why Does This Matter for Skin Cancer?
The reason dermoscopy is so valuable is that many of the features that distinguish a benign mole from a melanoma lie beneath the skin’s surface. Without magnification, even an experienced clinician can misclassify a dangerous lesion as harmless or unnecessarily remove one that poses no risk.
Studies have consistently shown that dermoscopy improves diagnostic accuracy for melanoma. A 2002 meta-analysis published in the Journal of the American Academy of Dermatology found that dermoscopy increased diagnostic sensitivity for melanoma by around 10 to 27% compared to the naked eye alone.
That might not sound dramatic, but in a disease where early detection is the difference between a simple excision and a complex treatment, it matters enormously.
What Is the Doctor Looking For?
The specific features a clinician evaluates depend on the type of lesion they’re looking at, but some of the key patterns include the following:
- Pigment network: a mesh-like pattern of lines caused by the distribution of melanin. An atypical network, one that’s irregular, broadened, or has abrupt endings, can be a warning sign.
- Regression structures: white scar-like areas or grey dots that suggest the body has been trying to break down abnormal cells
- Vascular structures: the patterns formed by small blood vessels. Irregular or looped vessels can indicate melanoma or other skin cancers
- Blue-white veil: a blue-white area overlying part of a lesion, which is associated with invasive melanoma
These features are assessed together, not in isolation. Dermoscopy is a clinical skill doctors spend years learning to interpret patterns accurately, and training significantly affects how useful the tool is.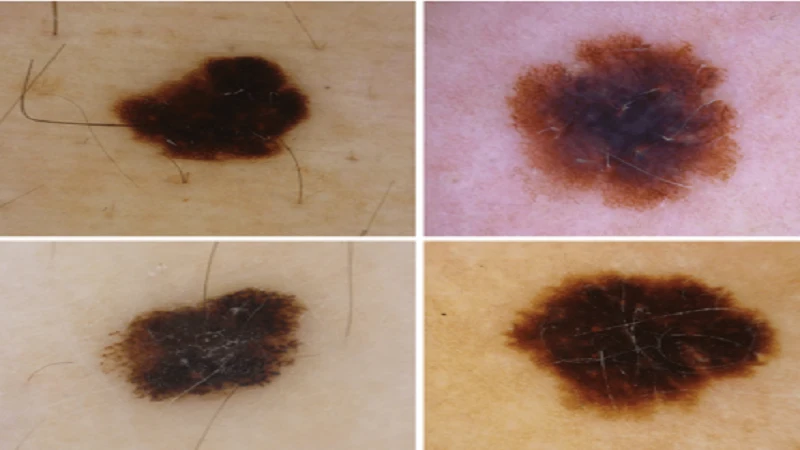
Alt text: Examples of dermoscopically and clinically equivocal MSLs from the case study (polarized dermoscopy, 20×) diagnosed histologically. Atypical nevi exhibiting an atypical network (A, B), a blue-white veil, and shiny white streaks (B). Early melanomas (C, D) showing only irregular dots and globules (C) and irregular pigmented blotches (D). Nevi were excised from the abdomen of a 43-year-old woman (A) and the arm of a 51-year-old man (B). Melanomas were excised from the upper back of an 83-year-old man (C) and a 79-year-old woman (D).”
What Are the Different Types of Dermatoscopes?
Dermatoscopes range from basic handheld models to sophisticated video dermoscopy systems used in mole mapping. At the handheld end, the two most widely used technologies are:
- Non-polarised contact dermoscopy: requires a liquid interface between the skin and the lens
- Polarised (non-contact) dermoscopy: uses cross-polarised light to eliminate reflection without contact gel
The DermLite DL5 handheld dermatoscope is a good example of what clinicians in Australia are currently using. It offers 10x magnification, a 32mm viewing area, and an integrated UV mode feature that make it versatile enough for both routine skin checks and more detailed lesion examination. Many doctors carry it in a coat pocket and use it for every patient.
Higher-end systems attach to cameras or computers, allowing images to be stored for comparison at future visits, which is the foundation of mole mapping.
Does Dermoscopy Hurt?
No. The dermatoscope is placed gently against the skin and produces no sensation. Some doctors use a small amount of ultrasound gel as a contact medium, which feels cool but isn’t uncomfortable. The entire examination of a single lesion typically takes 20 to 60 seconds.
Should You Ask Your Doctor About Dermoscopy?
If you’re having a skin check and your doctor isn’t using a dermatoscope, it’s completely reasonable to ask why. Not every GP is trained in dermoscopy, and not every clinic has the equipment. If your doctor isn’t able to perform a dermoscopic assessment, asking for a referral to someone who can is a perfectly sensible next step, particularly if you have many moles, a changing lesion, or a family history of melanoma.
Dermoscopy is one of the most practical advances in skin cancer detection of the last 30 years. It’s non-invasive, quick, and significantly improves the accuracy of diagnosis. If you’re seeing a doctor for a skin concern, knowing what the tool does and why it’s being used makes you a better-informed patient. See More
| You should know! |
| Dermoscopy has been shown to increase sensitivity for melanoma detection by up to 27% compared to examination with the naked eye alone. It is now considered a standard of care in dermatology and skin cancer medicine. |